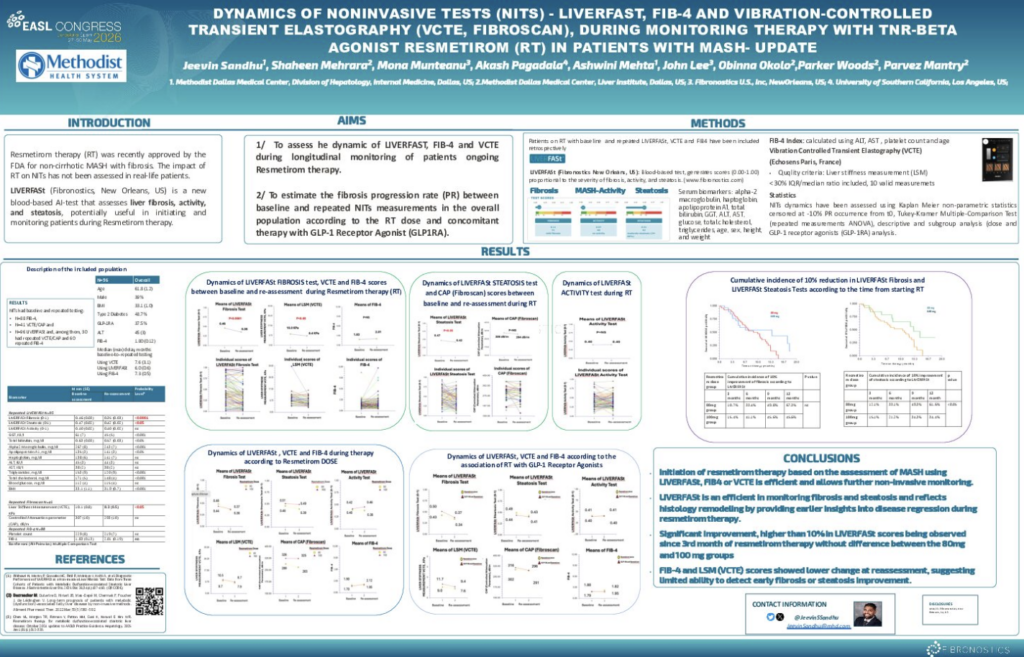
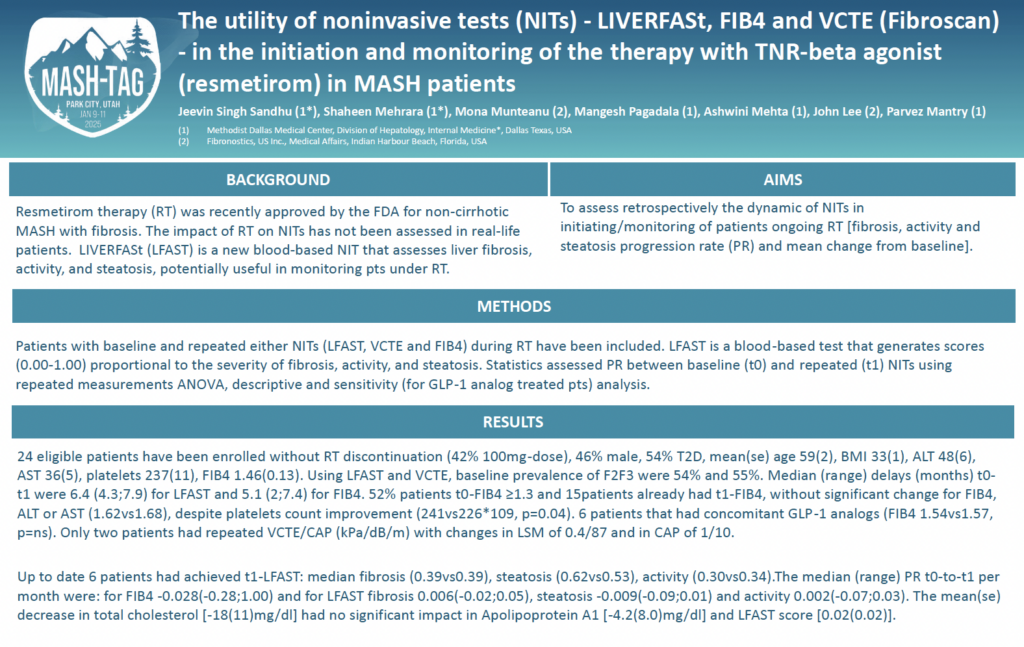
Dynamics of Noninvasive Tests (NITs) – LIVERFASt, FIB-4 and Vibration-Controlled Transient Elastography (VCTE, FibroScan), During Monitoring Therapy with Resmetirom (RT) in Patients with MASH
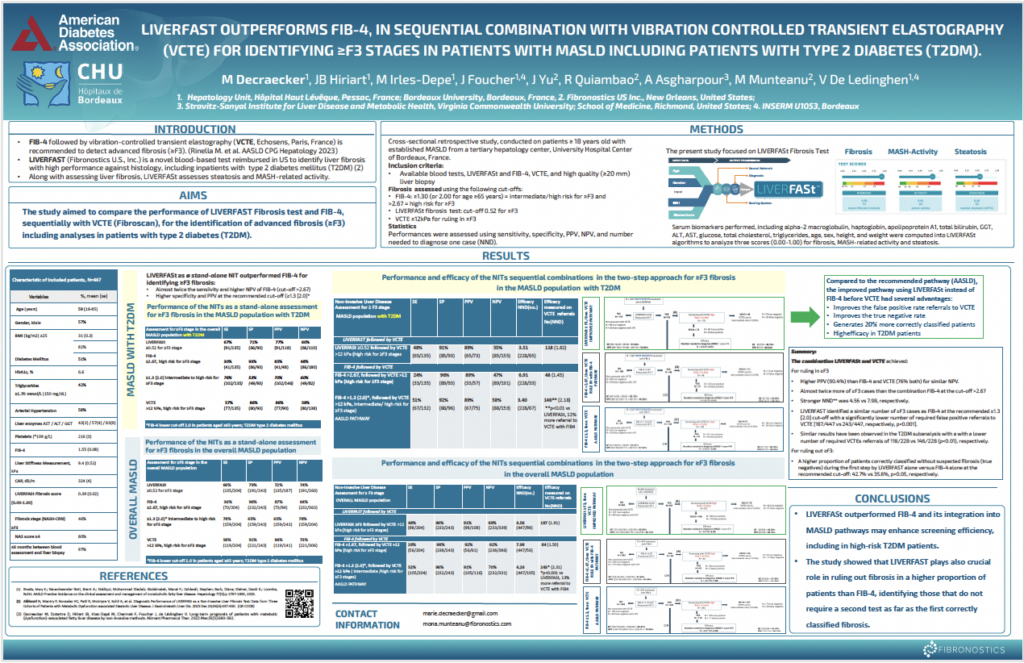
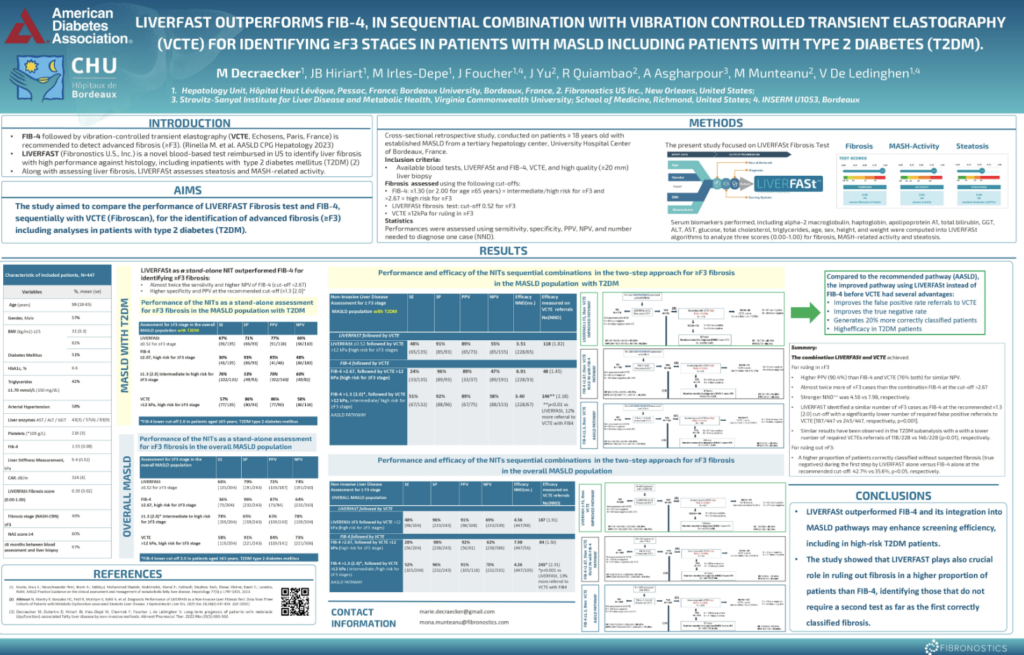
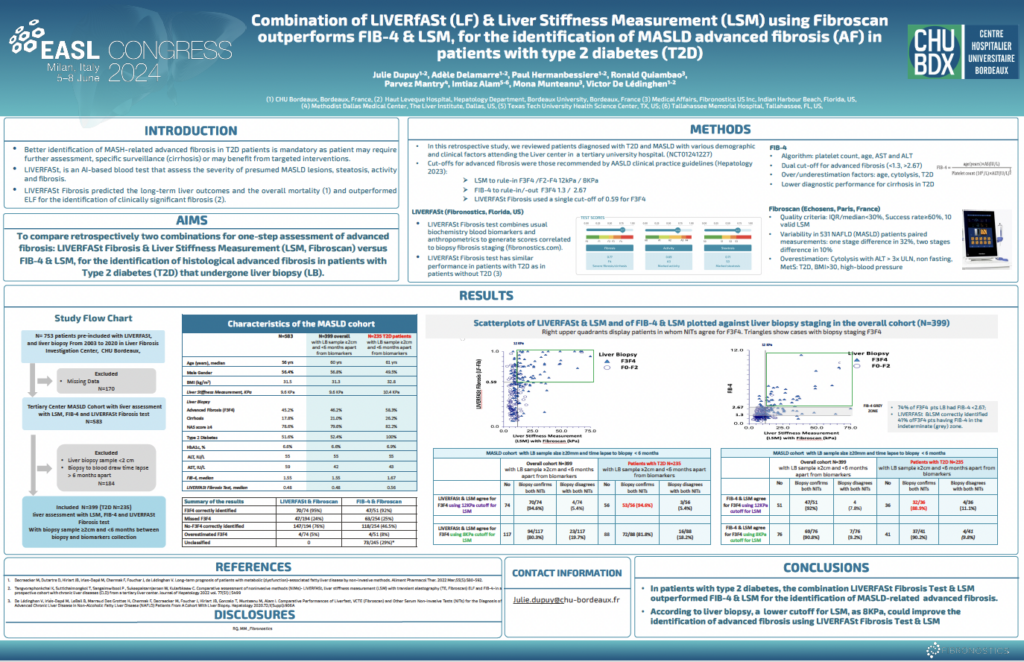
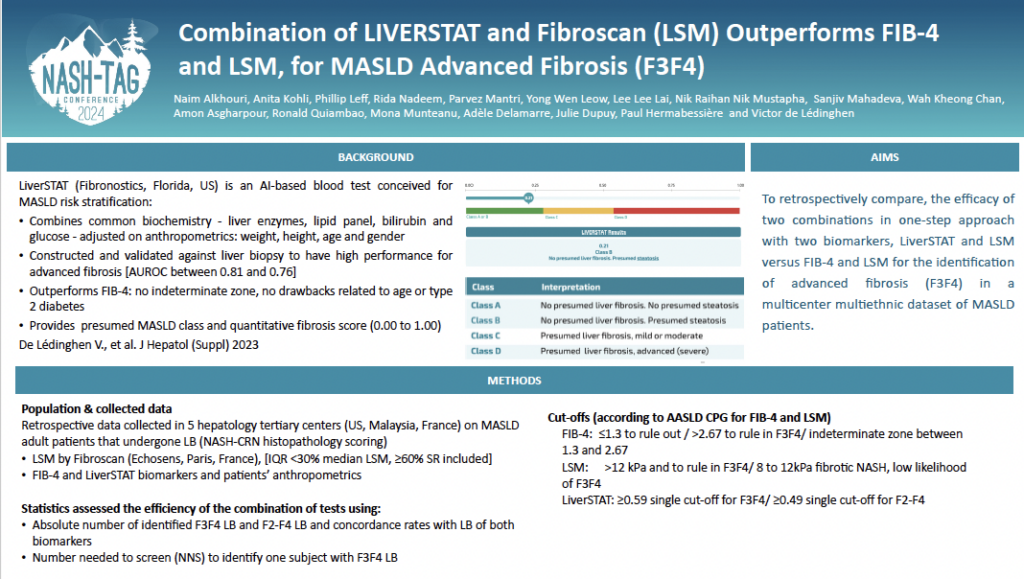
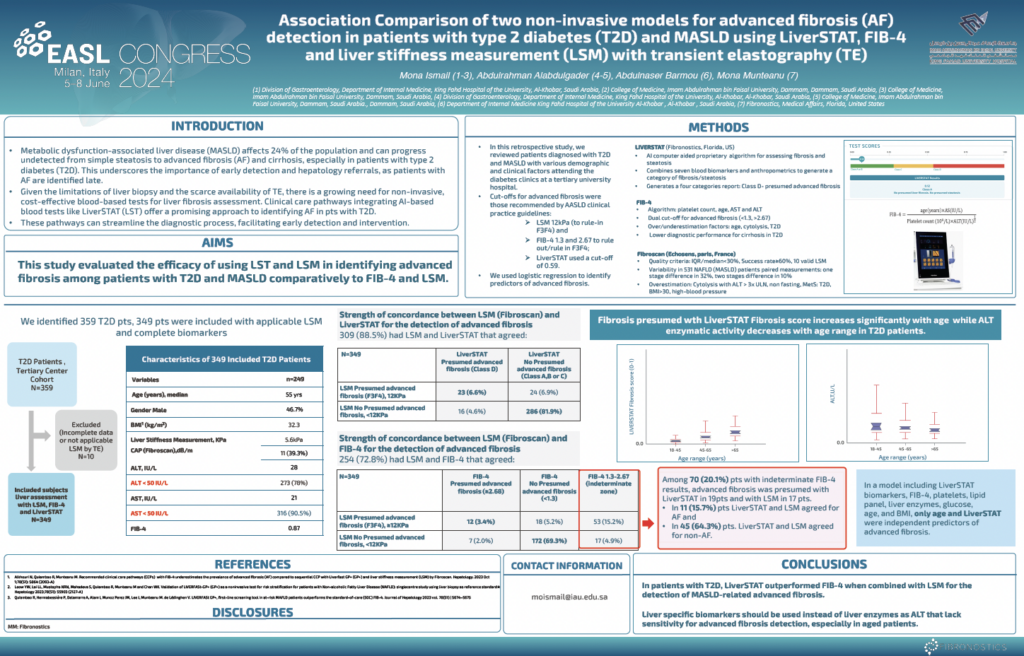
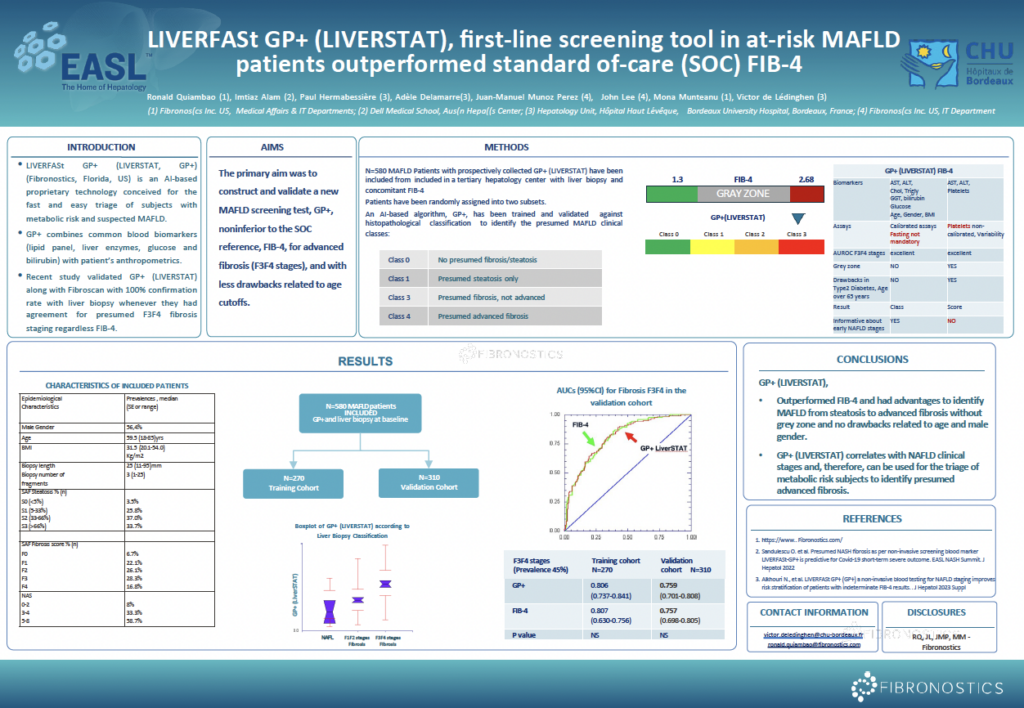
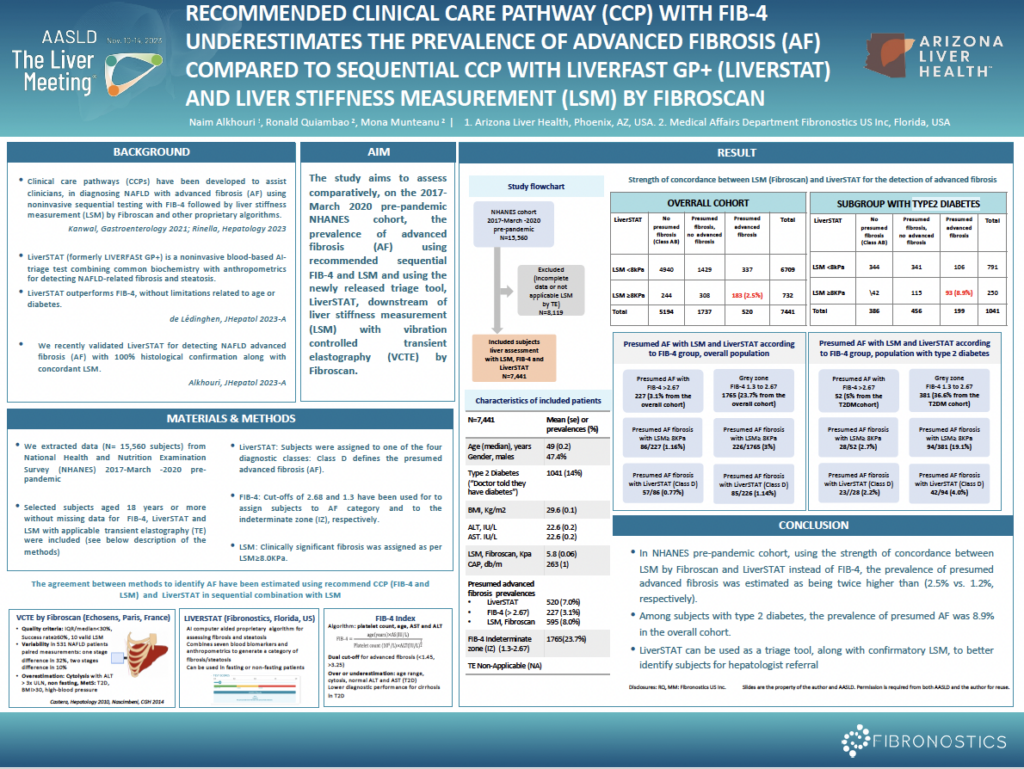
LIVERFASt Outperforms FIB-4, in Sequential Combination with Vibration-Controlled Transient Elastography (VCTE) for Identifying ≥F3 Stages in Patients with MASLD Including Patients with Type 2 Diabetes (T2DM)